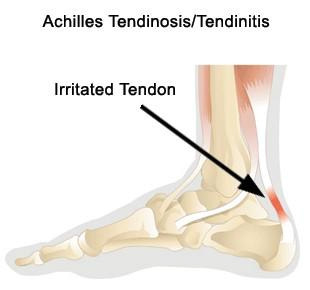
 The Achilles tendon (or heel cord) is the thick strap that can be felt running down the back of the calf into the heel. It is attached to, and worked by, the large muscles that make up the calf (gastrocnemius and soleus). When the Achilles tendon pulls on the heel it makes us go up on tiptoe, or pushes us forwards when walking or running. If this tendon is not working it is difficult to walk and the ankle feels weak.
The Achilles tendon (or heel cord) is the thick strap that can be felt running down the back of the calf into the heel. It is attached to, and worked by, the large muscles that make up the calf (gastrocnemius and soleus). When the Achilles tendon pulls on the heel it makes us go up on tiptoe, or pushes us forwards when walking or running. If this tendon is not working it is difficult to walk and the ankle feels weak.
Most Achilles tendon problems occur in middle-aged athletes and are basically overuse injuries. In a few cases, other medical conditions contribute to the weakening of the tendon. As we get older the tendon becomes less flexible and less able to absorb the repeated stresses of running. Eventually small “degenerative” tears develop in the fibres of the tendon. The body tries to repair these tears. Sometimes the repair process is successful. However, the blood supply of the lower part of the tendon is not very strong and the combination of this and the continued stresses of running mean that the tendon may not completely heal. Instead, the tendon and its lining become painful and swollen, and the tendon may feel weak. The combination of degenerative and repair processes in the tendon is called tendonosis (or sometimes tendonitis).
 Tendonosis develops gradually as the Achilles tendon and the heel become painful and a swelling may develop in or around the tendon. At first the problem is present mainly after running or playing sport, but later it may become increasingly difficult to walk because of the painful tendon.
Tendonosis develops gradually as the Achilles tendon and the heel become painful and a swelling may develop in or around the tendon. At first the problem is present mainly after running or playing sport, but later it may become increasingly difficult to walk because of the painful tendon.
Most people who have this problem will be treated with simple measures or physiotherapy and improve. A small number continue to have major problems which interfere with their lifestyle. In this situation an operation is indicated.
THE SURGERY
 If there is tenosynovitis (inflammation around the tendon) but the tendon itself is reasonably healthy, stripping out the inflamed tendon lining often gives good results. This can often be done telescopically with only small cuts in the skin. Often, however, the tendon itself is damaged and surgery would involve a bigger cut to remove the degenerate tendon and repair the remaining tendon. If the degenerate area is localised this can give quite good results. However, often the degeneration involves quite a lot of the tendon and removing it all may leave quite a large gap in the tendon which may need a major operation to repair. A big repair usually needs tendon borrowed from somewhere else, either higher up the Achilles tendon or from another tendon.
If there is tenosynovitis (inflammation around the tendon) but the tendon itself is reasonably healthy, stripping out the inflamed tendon lining often gives good results. This can often be done telescopically with only small cuts in the skin. Often, however, the tendon itself is damaged and surgery would involve a bigger cut to remove the degenerate tendon and repair the remaining tendon. If the degenerate area is localised this can give quite good results. However, often the degeneration involves quite a lot of the tendon and removing it all may leave quite a large gap in the tendon which may need a major operation to repair. A big repair usually needs tendon borrowed from somewhere else, either higher up the Achilles tendon or from another tendon.
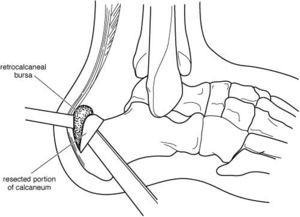
Sometimes, if the pain is located near where the tendon joins onto bone at the heel, a small piece of bone and other tissue may need to be removed as well. This to remove pressure off the tendon so that it can heal properly.
A plaster is applied. This is removed after 2 weeks. A walking boot (“moonboot”) is typically applied then.
CAN IT BE DONE AS A DAY CASE OPERATION?If you are otherwise fit, and there is someone who can collect you afterwards and stay with you overnight, the operation can be done as a day case. This means that you are admitted to hospital, operated on and discharged home on the same day. If you have other medical problems, or have no-one at home with you, you will have to stay overnight, and you may have to come into hospital the day before for medical tests or treatment. Some people find that they need to stay in hospital the night after surgery because the ankle is painful and they need strong pain killers. |
WILL I HAVE TO GO TO SLEEP (GENERAL ANAESTHETIC)?The operation is almost always done under general anaesthetic (asleep). Alternatively, an injection in the back can be done to make the ankle numb while the patient remains awake. Local anaesthetic injections do not always work and in that case you may have to go to sleep if the operation is to be done. The anaesthetist will advise you about the best choice of anaesthetic for you. In addition, local anaesthetic may be injected into your leg or foot while you are asleep to reduce the pain after the operation even if you go to sleep for the surgery. You will also be given pain-killing tablets as required. |
WILL I HAVE A PLASTER ON AFTERWARDS?Yes. This is only a half-plaster, to allow for swelling. |
FOLLOWING YOUR SURGERY
-
ON THE WARD
A heavy bandage or plaster splint down the back of your ankle and under your foot will be applied while you are asleep, as described above. You will be provided with crutches when you are discharged from hospital, and a physiotherapist will teach you how to use these.
-
WHEN YOU GO HOME
It is very important that the leg remains elevated most of the time in the first 2 weeks – rest is important. Do not wet or remove the plaster. It is normal to expect:
It is normal to expect:
-
SWELLING – This can be minimised by elevating your foot above your heart; icing the foot may be helpful
-
PAIN – You will receive a prescription for pain medication on discharge from hospital. Pain can also be minimised by elevating your leg.
-
BLEEDING – This always occurs. You may notice some oozing through the bandages.
Do not put any weight through your leg for the first 2 weeks.
Further AppointmentsYou will be seen in Dr Sterling’s rooms 12-14 days after your operation. The plaster will be removed and the wound inspected. Your rehabilitation will be customised from here, but may involve a further period of immobilisation or early physiotherapy. Dr Sterling will advise you at this appointment. You will be seen regularly after this to ensure that the tendon is healing, and that physiotherapy is improving the situation. |
HOW SOON CAN I….
-
GO BACK TO WORK?
If your ankle is comfortable, you can work in a plaster and sit with your foot up most of the time (basically in a desk job), you could go back to work within a few weeks of surgery. On the other hand, if you do a heavy manual job you may need two or three months off work or longer. How long you are off will depend on where your job fits between these two extremes.
-
DRIVE?
If you have your left foot operated on and have an automatic car you can drive within a few days of the operation, when your foot is comfortable enough. Otherwise you will have to wait until the ankle is strong and flexible enough to work the pedals, especially in an emergency situation. This will probably not be for 6-8 weeks after surgery.
When you return to driving you need to take it gradually at first and drive only short distances. Also remember that if you drive before you can stop or manoeuvre in an emergency your insurance will not cover you in the event of an accident.
-
PLAY SPORT?
You can gradually increase your level of activity under the guidance of your physiotherapist. Once you can walk comfortably you can start walking, swimming and cycling, increasing the distance covered gradually. As this recovers you can go back to low-impact, non-contact sports and finally to full contact sports. It is common to take 9-12 months at least to return to sports such as football or rugby.
IF YOU ARE CONCERNED:
|